Evaluating patients with stable chest pain remains one of the most common and debated challenges in cardiovascular care. While coronary CT angiography (CCTA) is widely used for its high sensitivity and negative predictive value, its moderate positive predictive value (60–70%) often leads to additional downstream testing.
This creates a familiar clinical dilemma:
- Which patients truly need further testing?
- How can unnecessary invasive procedures be avoided?
- Can we improve efficiency without compromising care?
A recent interventional simulation study from investigators at Hospital Álvaro Cunqueiro and the Cardiovascular Research Group at IIS Galicia Sur (Vigo, Spain), including José A. Parada-Barcia, Manuel Barreiro-Pérez, and Andrés Íñiguez-Romo, explored the potential clinical and economic impact of incorporating FFR-CT into the diagnostic pathway for moderate CAD.
While these findings are hypothesis-generating rather than definitive, the study offers encouraging real-world insights into the potential value of FFR-CT-guided care in appropriately selected patients, including:
- Lower diagnostic costs
- Improved clinical confidence in decision-making
- Higher discharge rates, potentially reducing downstream testing
In this analysis, the FFR-CT assessments were performed using DEEPVESSEL FFR, a deep learning–based platform, reflecting the continued evolution of AI-enabled cardiovascular imaging.
Study Overview
Clinical and economic impact of FFR-CT–guided management in moderate coronary artery disease: an interventional simulation study
- Population: 43 patients with moderate coronary stenosis (50–69%)
- Design: Retrospective, single-center simulation
- Method: 5 cardiologists evaluated each case:
- With CCTA alone
- With CCTA + FFR-CT
- Tool used for FFR-CT: Deep learning-based software (DeepVessel FFR). The study simulated real-world decision-making to understand how functional data impacts clinical pathways.
Key Findings
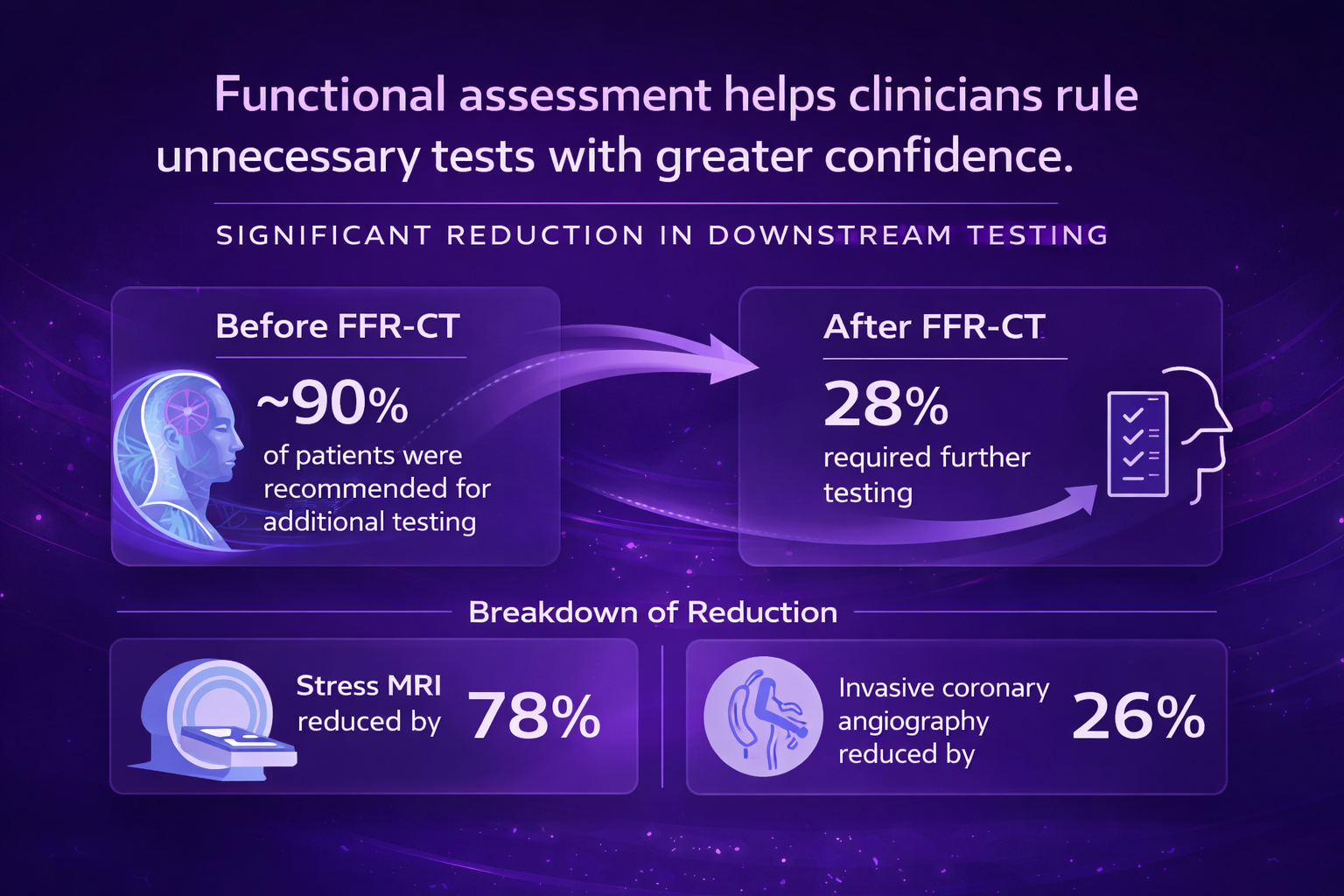
1. Significant Reduction in Downstream Testing
- Before FFR-CT: ~90% of patients were recommended for additional testing
- After FFR-CT: FFR-CT helped reduce further testing recommendations to just 28% in simulated clinical scenarios.
- Breakdown:
- Stress MRI reduced by 78%
- Invasive coronary angiography was reduced by 26%
2. Diagnostic costs decreased after incorporating DVFFR, driven by reduced downstream testing.
DVFFR-guided care was associated with lower diagnostic costs, more patients being discharged without further testing, and high perceived clinical utility among physicians. Even after accounting for the approximate €400 cost per FFR-CT analysis, the strategy reduced total cost per patient by about €214 and generated roughly €46,000 in total cohort savings. It also increased the discharge rate from 11% to 48%, while physicians rated DVFFR as clinically useful in approximately 80–87% of cases.

Figure 1. Study design and outcomes. CAD-RADS, coronary artery disease-reporting and data system; CT, computed tomography; FFR, fractional flow reserve; ICA, invasive coronary angiography; MRI, magnetic resonance imaging.
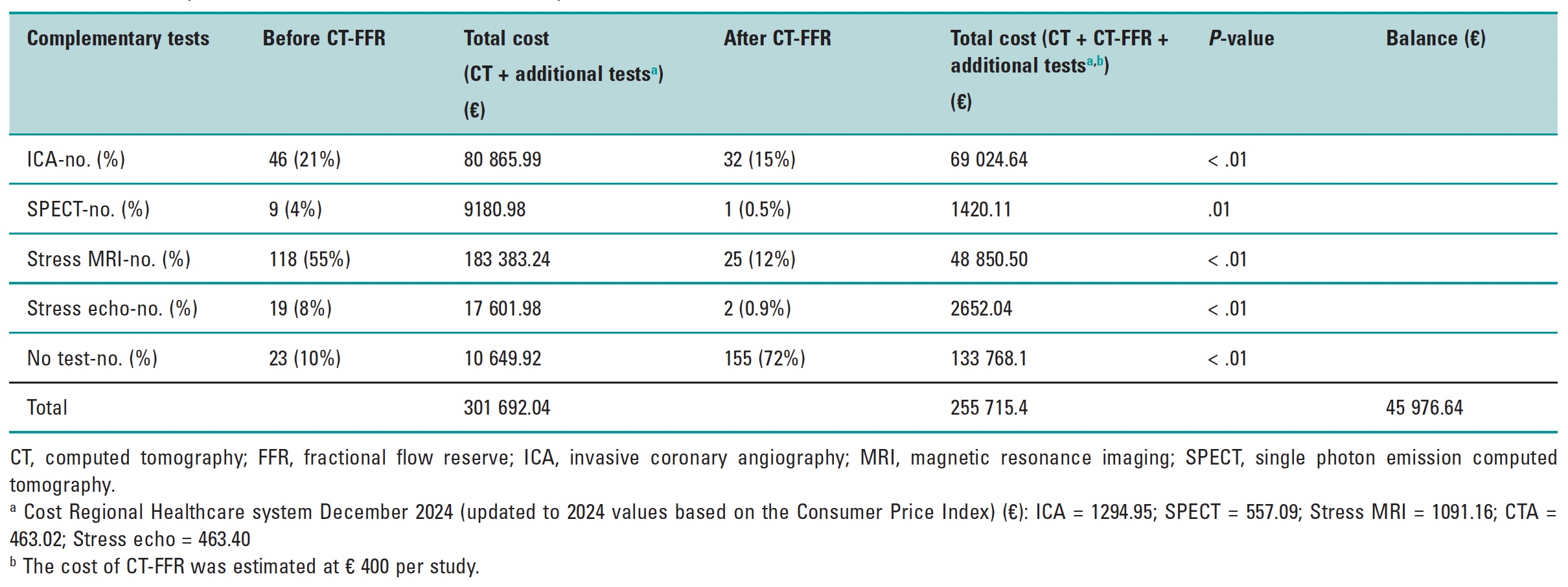
Table 1. Cost analysis based on clinical simulation analysis
The Role of AI in FFR-CT in Clinical Practice
Acknowledging that these results are hypothesis-generating rather than definitive, this study adds encouraging real-world evidence on the potential clinical and economic value of FFR-CT-guided care, such as:
- Lower diagnostic cost
- Improve clinical confidence
- Increase discharge rates
The FFR-CT analysis in this study was performed using DEEPVESSEL FFR, a deep learning–based platform, reflecting a broader shift toward AI-enabled cardiovascular imaging. AI-based FFR-CT solutions can help reduce reliance on additional stress testing in appropriately selected patients, provide vessel-level functional insights, and easily integrate into existing CCTA workflows. As these technologies evolve, they may play an increasing role in scaling advanced cardiac imaging in routine clinical practice.
References
- Parada-Barcia JA, et al. Clinical and economic impact of FFR-CT–guided management in moderate coronary artery disease: an interventional simulation study. REC Interv Cardiol. 2026.